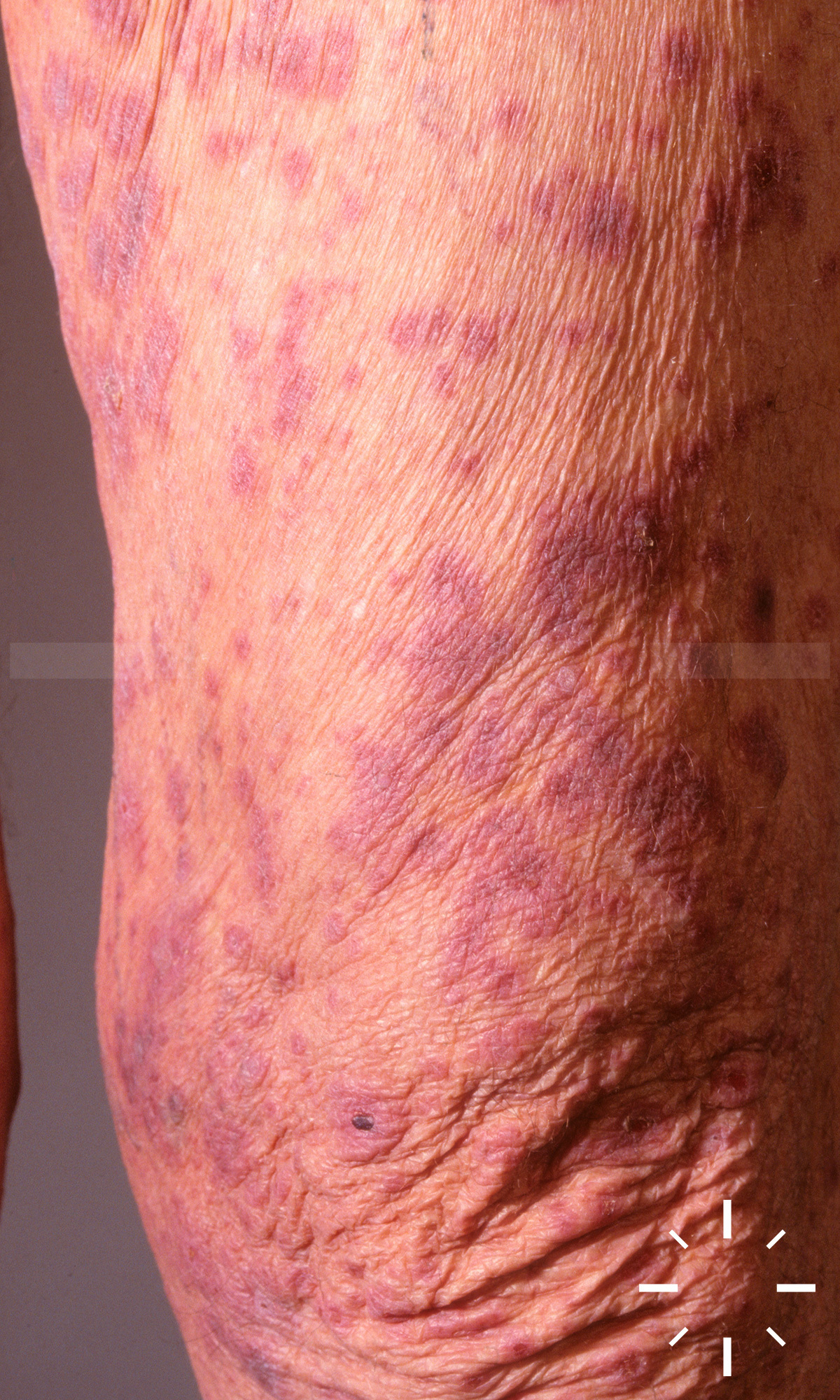
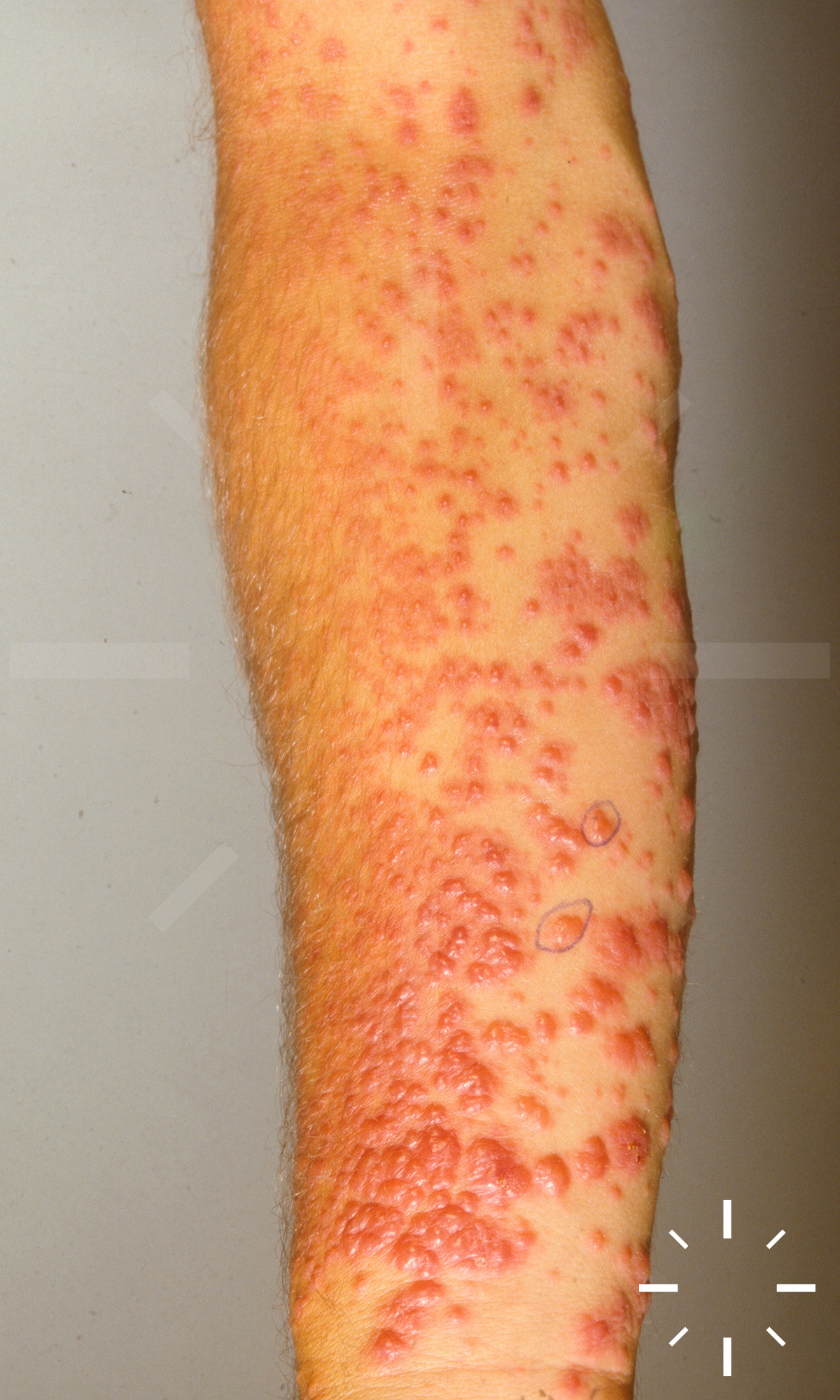
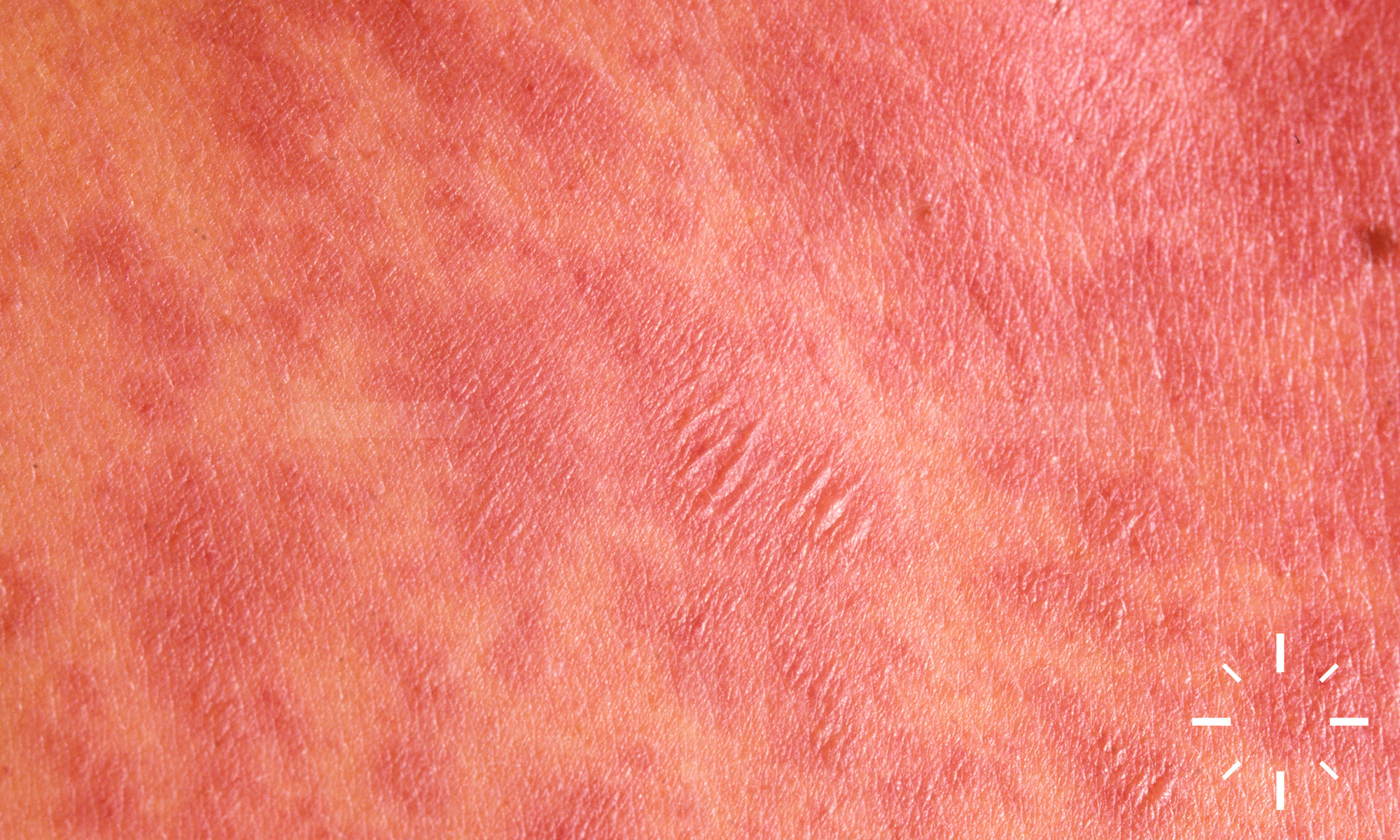
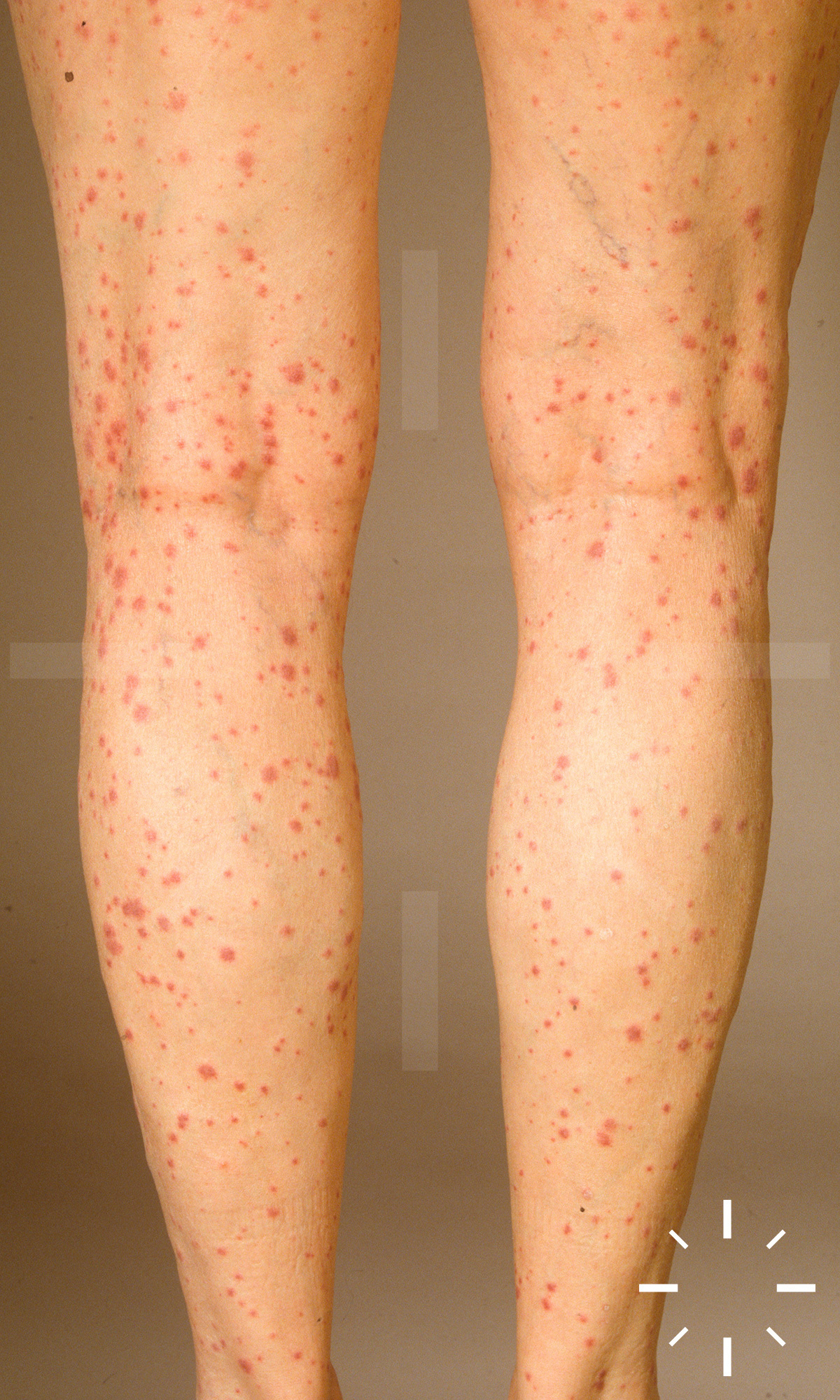
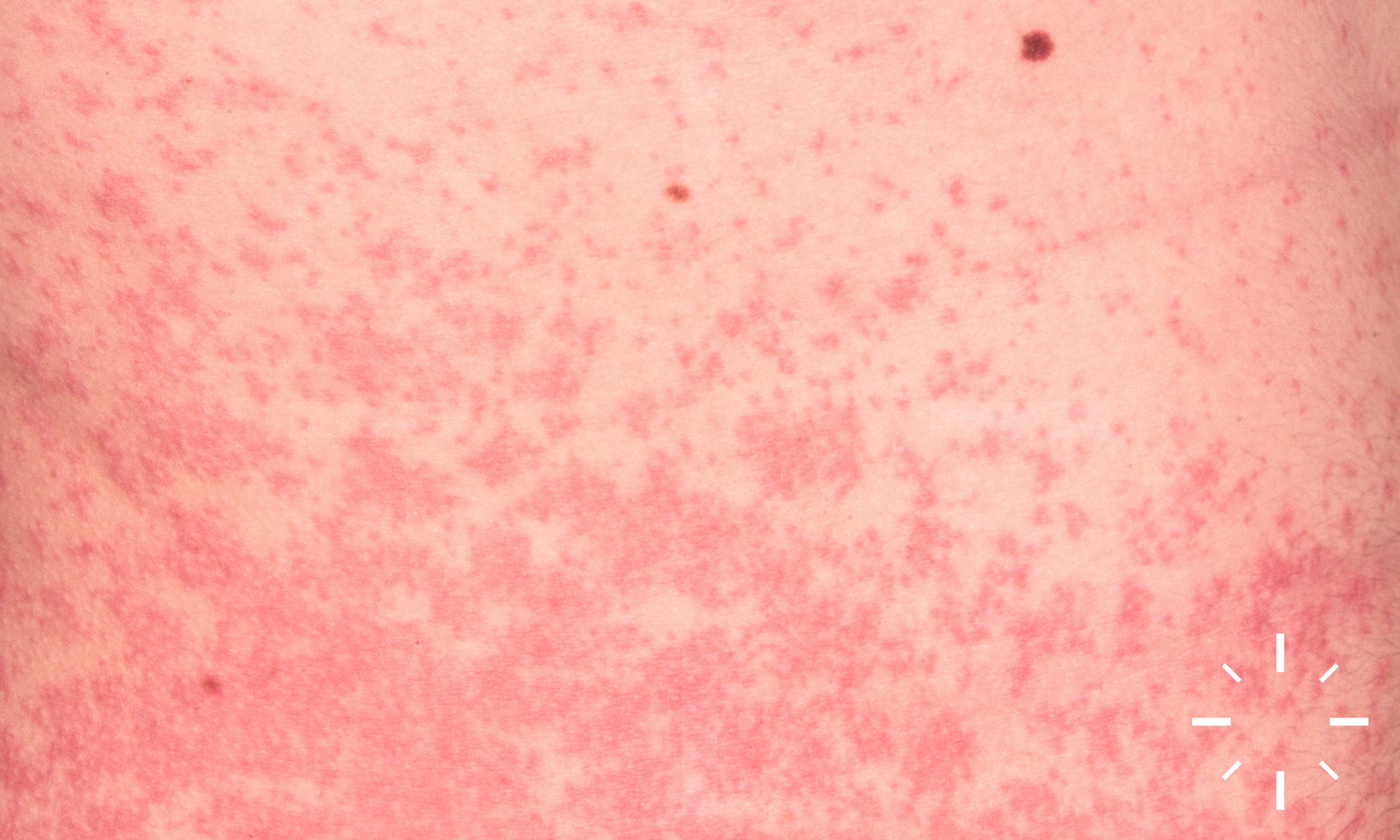
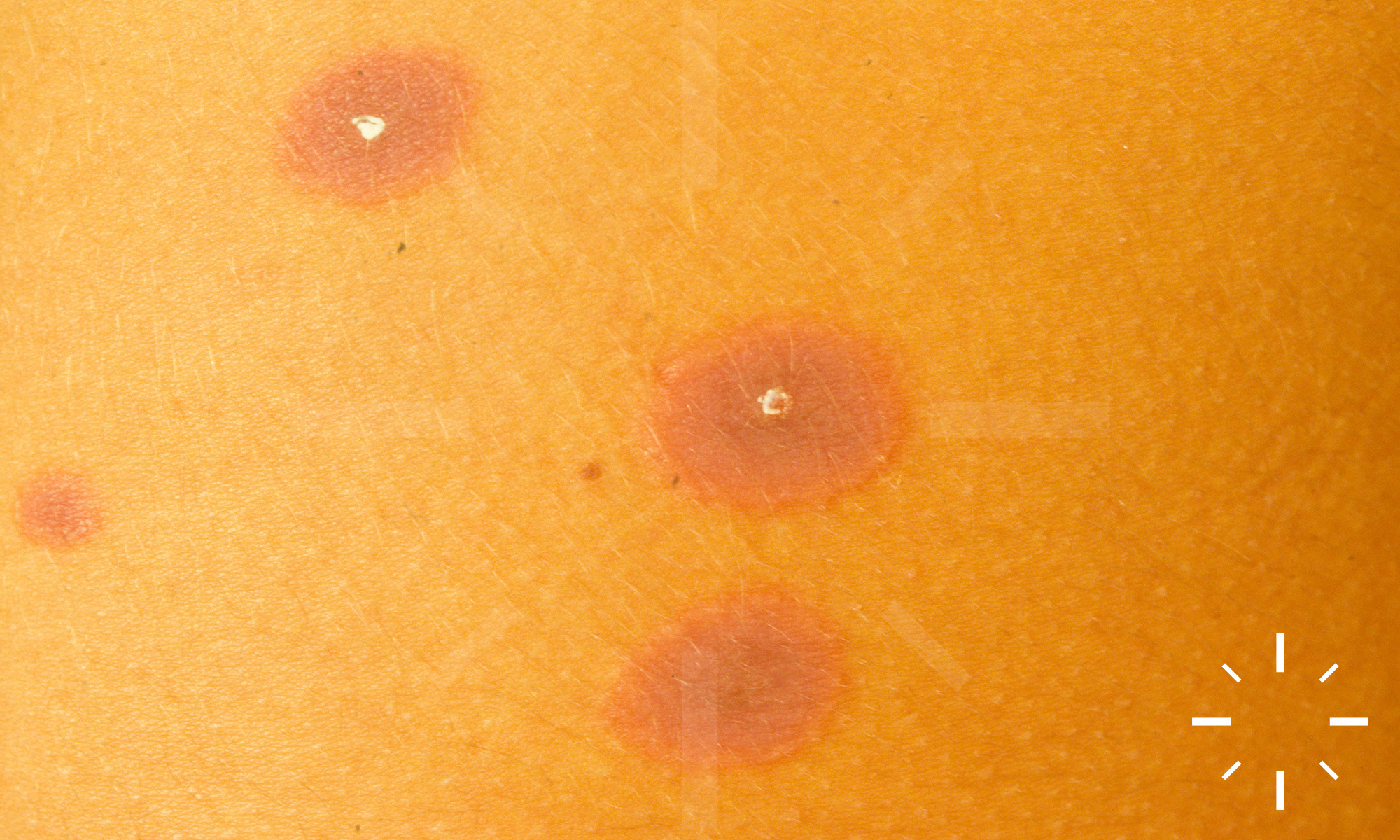
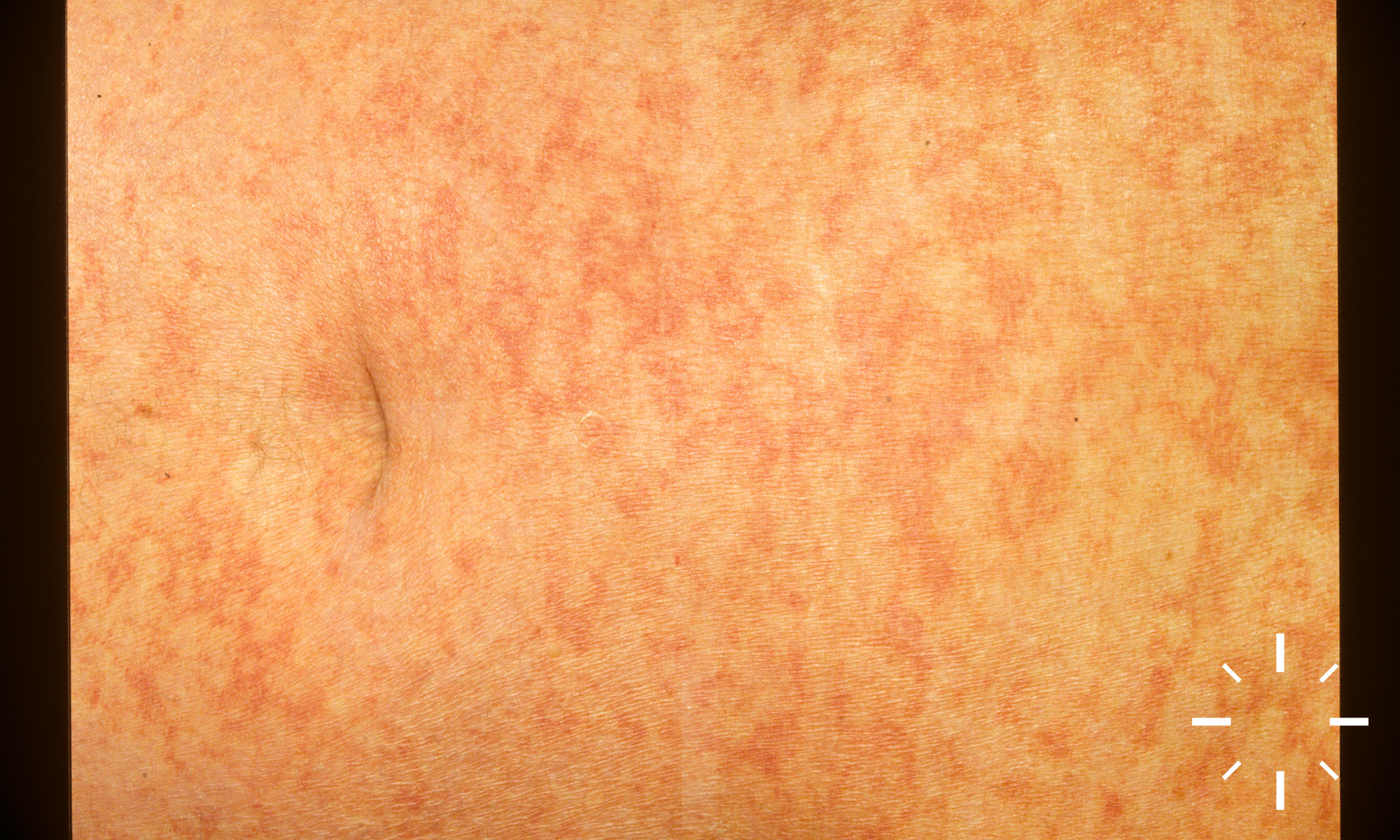
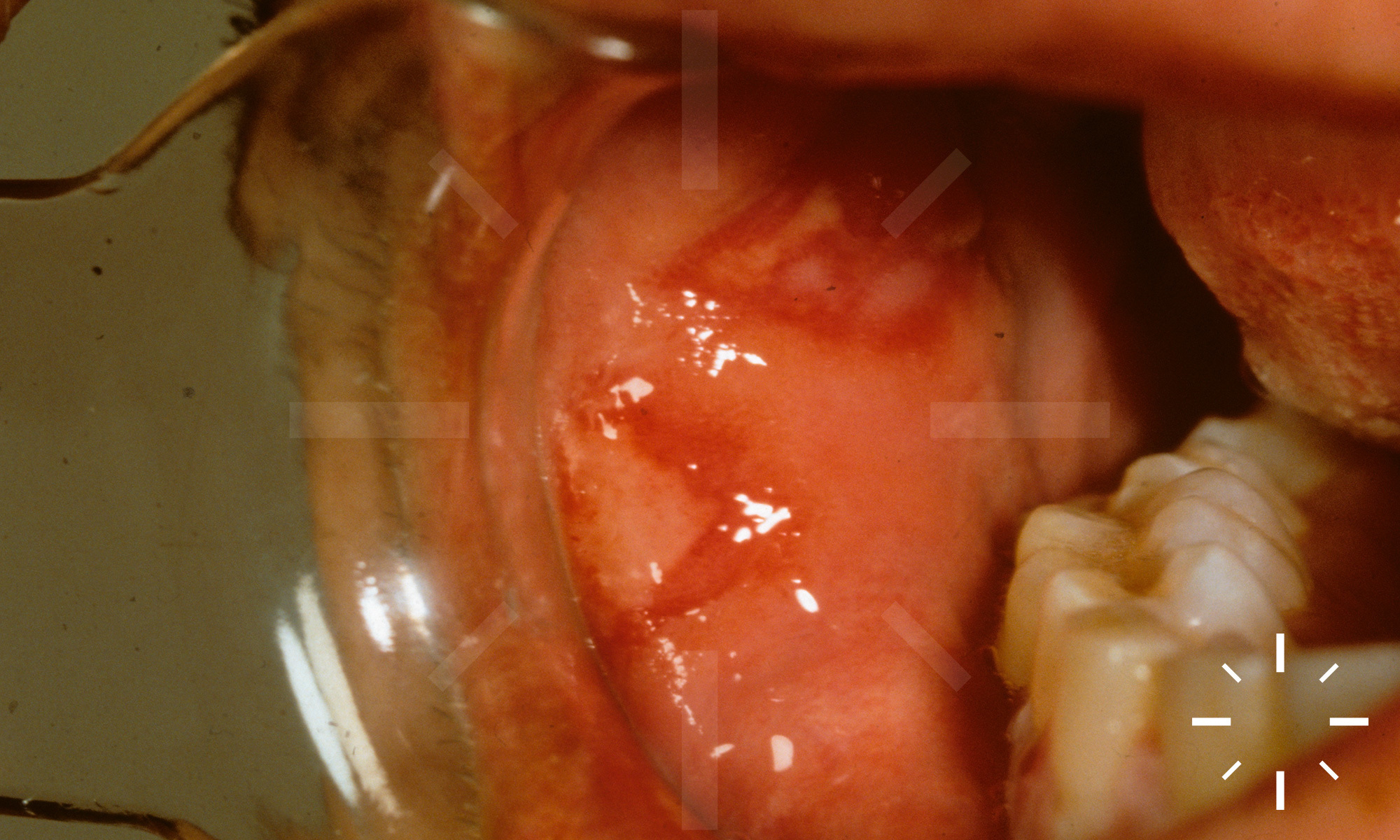
Erythema exsudativum multiforme
Last Updated: 2025-02-11
Author(s): Anzengruber F., Navarini A.
ICD11: EB12.Z








































































1/80