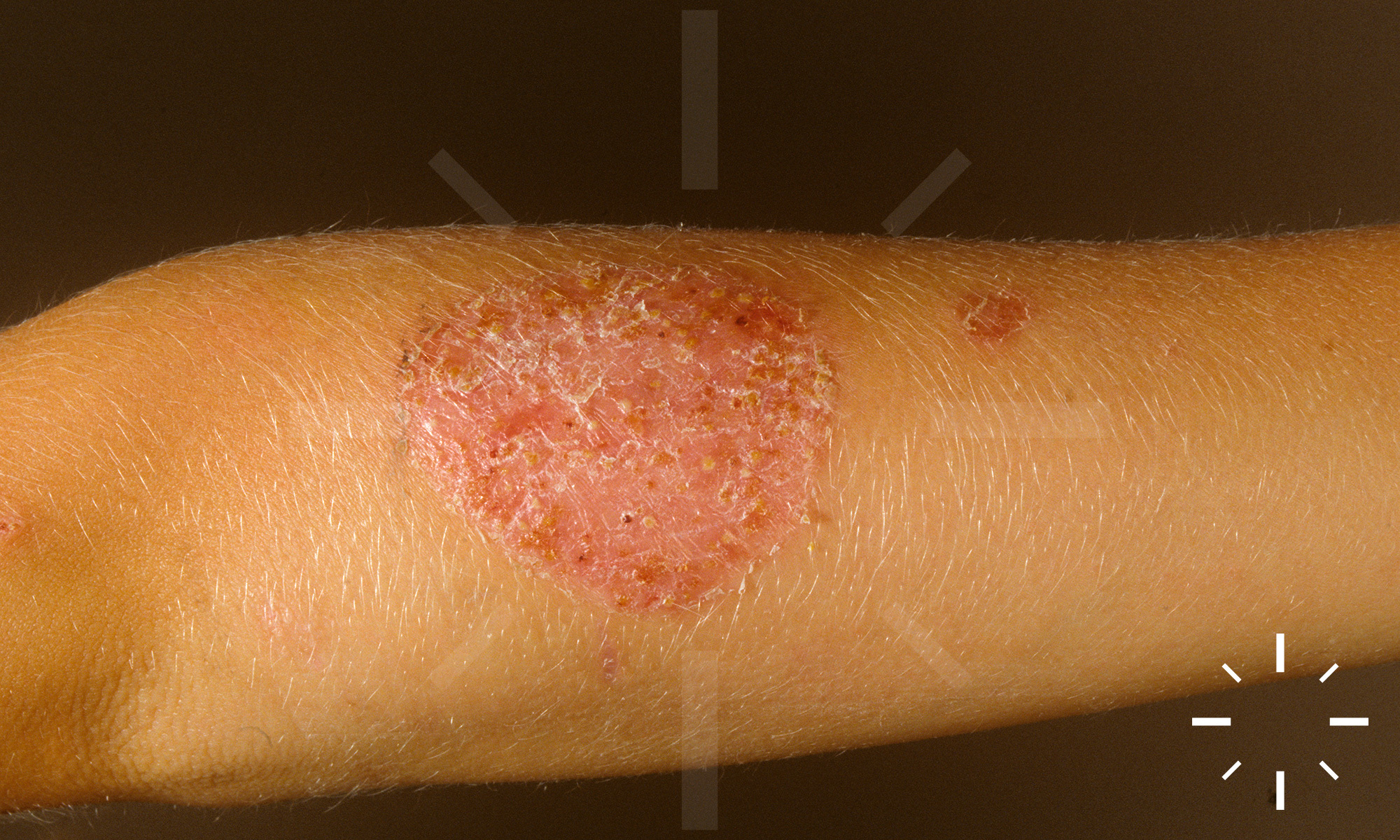
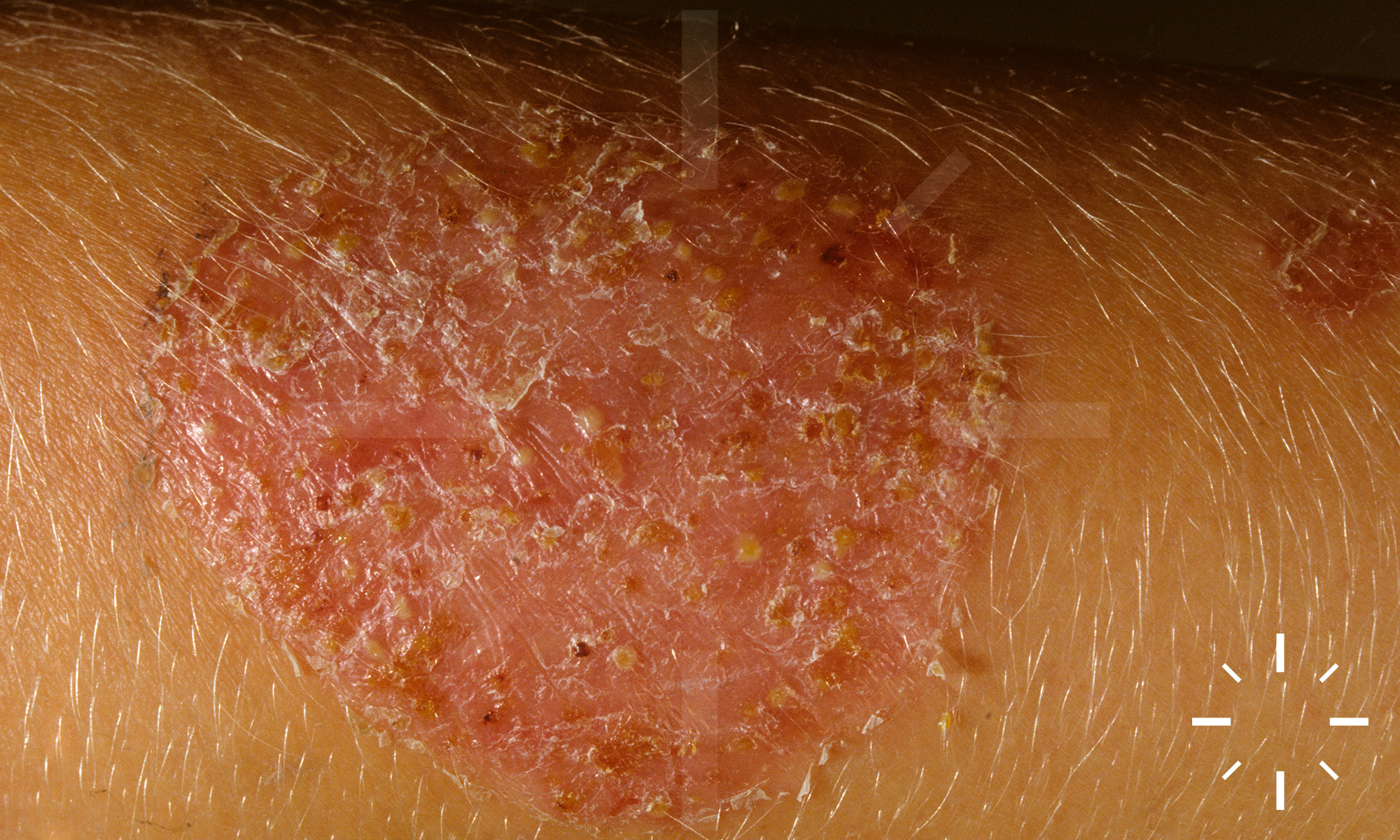
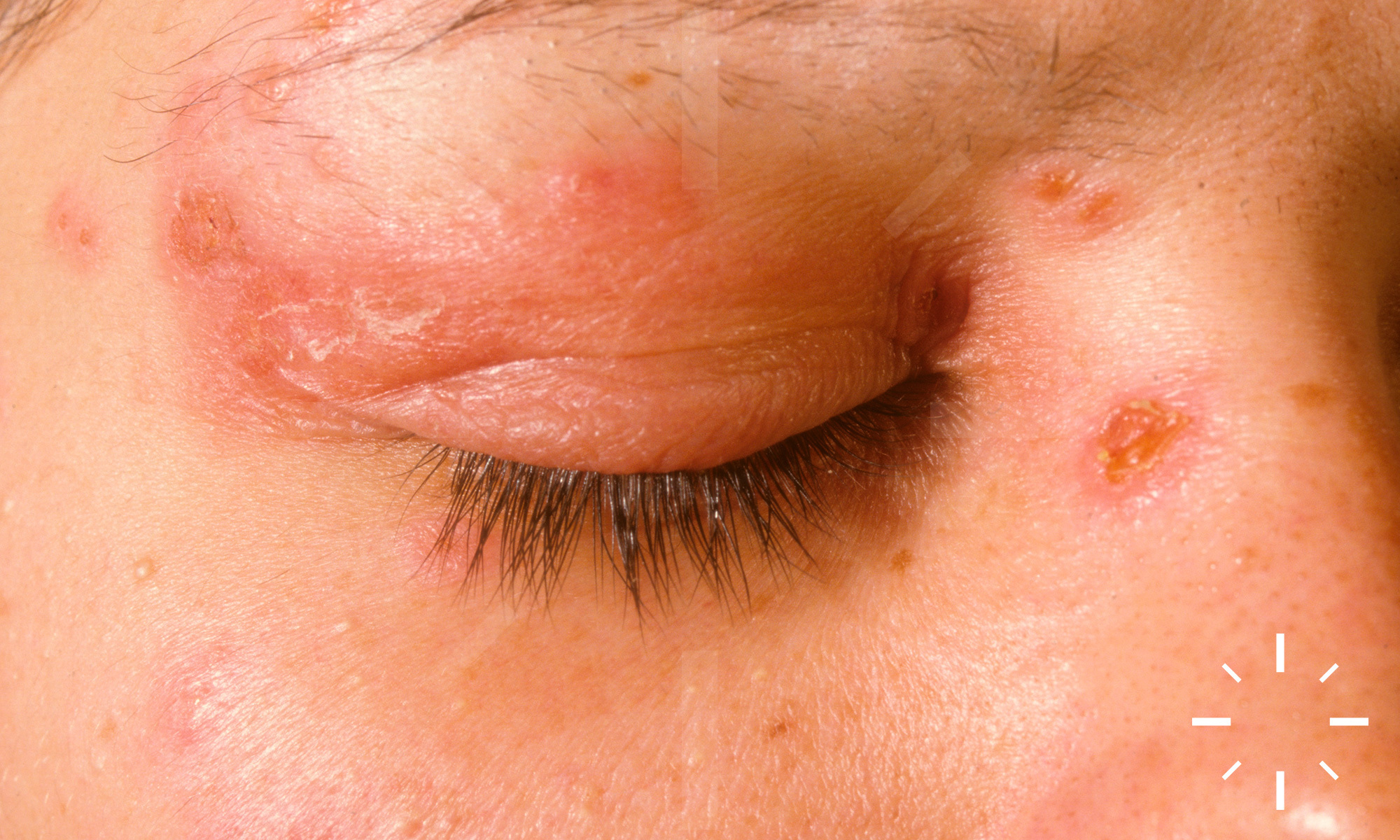
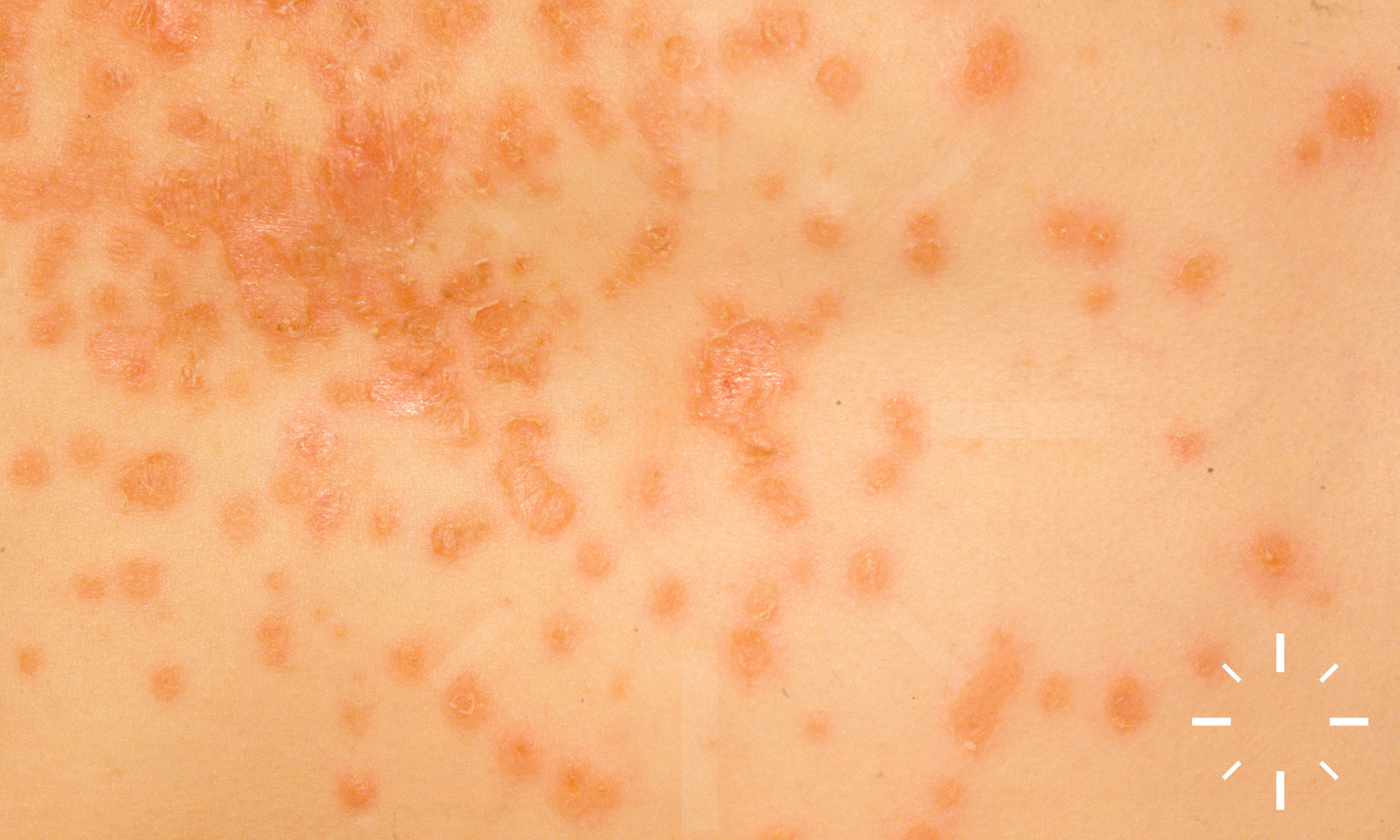
Impetigo contagiosa
Last Updated: 2023-07-07
Author(s): Anzengruber F., Navarini A.
ICD11: 1B72.Z


























1/30